
Overview
What is a spinal CSF leak?
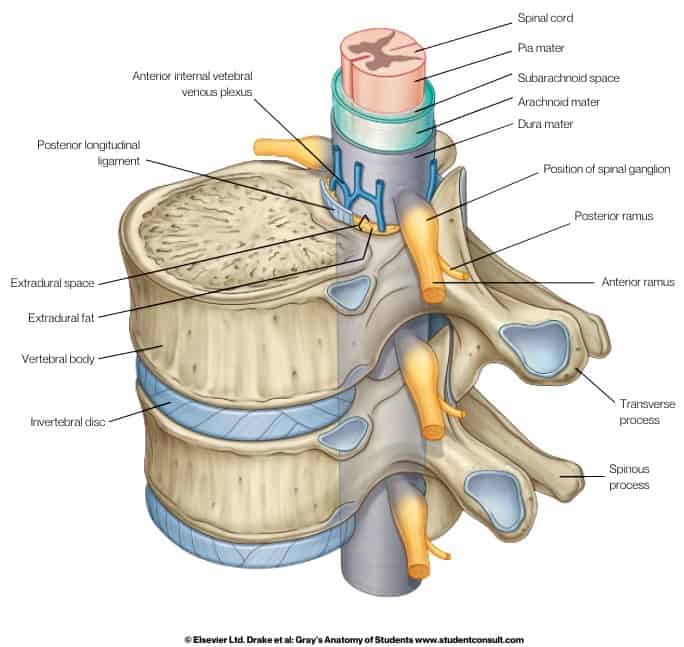
The brain and spinal cord are bathed in fluid known as cerebrospinal fluid (CSF). This fluid is held inside layers of connective tissue called the meninges, which surround the brain and spinal cord. There are three meningeal layers: the pia mater; the arachnoid mater; and the dura mater. The dura mater, sometimes called the dura, is the outermost layer of the meninges. The dura is normally a tough connective tissue. The CSF is contained within the subarachnoid space, between the arachnoid mater and the pia mater layers. A spinal CSF leak happens when the spinal dura mater has a hole, tear, or other defect, allowing cerebrospinal fluid (CSF) to leak out of this enclosed space. This results in intracranial hypotension, a low volume of CSF remaining around the brain and spinal cord.
This image shows the basic anatomy of the spinal cord with meningeal layers.
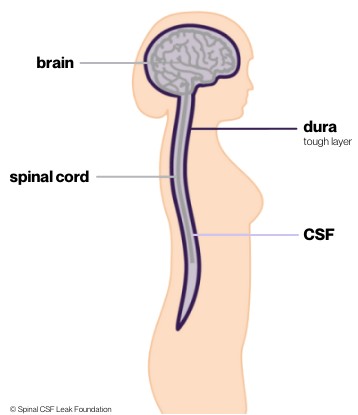
This image shows the brain, spinal cord, and dura, and illustrates that the cerebrospinal fluid flows around both the brain and the spinal cord in one compartment.
What are the symptoms of spinal CSF leak?
The loss of volume of CSF around the brain and spinal cord can result in a range of symptoms, with severe positional headache being the most common. Symptoms can be mild to very disabling. Often, a patient may have very limited ability to function while in the upright position. A wide range of neurologic signs and symptoms may occur, and rarely, dementia, stroke, coma, and even death have been reported.
What causes a spinal CSF leak?
Dural holes or tears can happen due to a number of reasons, whether iatrogenic, traumatic, or spontaneous.
Iatrogenic spinal CSF leaks are caused by a medical procedure, intentionally or inadvertently. These occur at the time of a spinal tap (lumbar puncture), which is a diagnostic sampling of CSF, or at the time of a lumbar puncture for injection of contrast for a type of spinal imaging known as myelography. Most often these holes heal over quickly, but in some cases they do not. Dural tears may occur inadvertently at the time of epidural injections (epidural refers to the space in the spinal canal outside of dura and spinal cord). They may also occur at the time of surgery.
Traumatic spinal CSF leaks are caused as a result of an injury.
Spontaneous spinal CSF leaks occur with minimal or no clear precipitant. Often, these spontaneous leaks are associated with thinner dura than normal, as is seen with a number of heritable disorders of connective tissue. A dural tear may also be caused by a calcified intervertebral disc or bone spur.
How is it diagnosed?
The diagnosis may be suspected on the basis of symptoms. MRI of the head, without and with contrast, is the diagnostic imaging that should be performed in most cases. There are several typical findings seen in 80 % of cases, although normal imaging does not rule out the diagnosis.
Spinal imaging, including myelography, is used to locate the CSF leak. This can be done using magnetic resonance imaging (MRI), computed tomography (CT), or digital subtraction imaging. Spinal imaging fails to identify leaks in about half of suspected cases due to limited sensitivity, which impacts treatment options.
How is it treated?
Initial treatment may be conservative if the symptoms are not severe. This might include bedrest, oral and IV fluids, and oral and IV caffeine. Some cases resolve without any further treatment. For those that require treatment, epidural patching with autologous blood (the patient’s own blood) is the mainstay of treatment. This can be repeated a number of times. Epidural patching with fibrin glue can be directed at specific leak locations. A percentage of patients will require surgical repair by a spinal neurosurgeon.
What is the prognosis?
Misdiagnosis or delayed diagnosis of spontaneous spinal CSF leak is common and is largely related to a lack of familiarity among physicians. Unfortunately, the degree of disability may also be underestimated, contributing to a delay in appropriate diagnostic testing and treatment.
Overall, the prognosis is good for the majority of patients with appropriate diagnostics and treatments, although some patients continue to have persistent symptoms despite several procedures.