
Diagnosis
Diagnosing a Spinal CSF Leak
Recognizing and diagnosing spinal CSF leak can be challenging, largely due to low familiarity on the part of health care professionals. Read on for more information on the importance of patient history in the diagnosis of spinal CSF leak, recognizing physical signs of a spinal CSF leak, challenges in diagnosing spinal CSF leak, diagnostic testing, diagnostic imaging, diagnostic findings, types of spontaneous spinal CSF leak, and diagnostic criteria for spontaneous spinal CSF leaks.
The Importance of Patient History in the Diagnosis of Spinal CSF Leak
The most important clues to the diagnosis of intracranial hypotension lie in the patient history.
SYMPTOMS
The hallmark symptom is head pain that is worse when upright and improved with horizontal positioning. It is important to note that not all headaches related to spinal CSF leaks are positional, and not every patient with a positional headache has a spinal CSF leak. Common and uncommon associated symptoms are listed on our Symptoms page.
HISTORY OF MEDICAL PROCEDURES OR TRAUMA
Lumbar punctures, epidural injections and spinal surgery occurring prior to onset of symptoms may be responsible for a spinal CSF leak. Significant trauma may also result in a spinal CSF leak. See our page on Causes.
HISTORY OF HERITABLE DISORDERS OF CONNECTIVE TISSUE (HDCT)
Spinal CSF leaks that develop spontaneously or with minimal precipitant may be related to an underlying weakness of the spinal dura. Marfan Syndrome, Ehlers-Danlos Syndrome, and other HDCTs, as well as Polycystic Kidney disease, have been associated with spontaneous leaks. In many cases, the symptoms related to intracranial hypotension are the first recognized evidence of a HDCT.
KNOWN SPINAL PROBLEMS
Spontaneous leaks are also associated with calcified discs or bone spurs that may or may not be known prior to the onset of symptoms.
PREVIOUS DIAGNOSIS OF POTS (POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME)
The poor tolerance of upright posture associated with POTS can mimic intracranial hypotension, but the two may also coexist. Patients with the hypermobile type of Ehlers-Danlos Syndrome are known to have a higher prevalence of POTS, as well as a greater risk of spontaneous intracranial hypotension.
PREVIOUS DIAGNOSIS OF CHIARI
Low-lying cerebellar tonsils on cranial imaging can be the result of intracranial hypotension (and fully reversible) and may not be recognized as such. To complicate matters, congenital Chiari is also more common in patients with some types of HDCT.
Physical Signs of a Spinal CSF Leak
EVIDENCE OF HDCT
There are a number of physical signs of HDCT that may be noted, such as joint hypermobility, high arched palate, dental crowding, tall stature, scoliosis, easy bruising, atrophic scars, and a number of others.
NEUROLOGIC FINDINGS
There are many findings, including involvement of cranial nerves, cognitive changes, gait disturbance, and sensory and motor changes, but the exam may be entirely normal.
CLINICAL MIMICS
There are a number of disorders that intracranial hypotension may mimic due to the wide range of neurologic presentations. Patients may present with dementia, ataxic gait, Parkinsonism, and other movement disorders.
SERIOUS NEUROLOGIC PRESENTATIONS
Emergency Medicine physicians may see patients presenting clinically with quadriplegia, stupor, coma, or other serious neurologic presentations. Death is a reported complication, albeit rare.
Challenges in Diagnosing Spinal CSF Leak
Misdiagnosis and delayed diagnosis of spinal CSF leak remain common, largely due to low familiarity by health care professionals, as we see with all uncommonly recognized disorders. There is considerable variability in clinical presentations and many diagnostic challenges. Severity of symptoms and degree of disability are often underappreciated. Not surprisingly, many patients suffer for months or years before a correct diagnosis is made.
Diagnoses often considered
- Primary headache disorders such as migraine headache, tension headache
- Sinus headache
- Cervicogenic headache (arising from neck problems)
- Meningitis
- Occipital neuralgia, trigeminal neuralgia
- New daily persistent headache
- Post-traumatic headache (post-concussion or whiplash)
- Psychogenic disorder (arising from psychological issues), depressive disorder, anxiety disorder
Differential or concurrent diagnoses
- POTS (postural orthostatic tachycardia syndrome) may be an alternate or concurrent diagnosis
- Chiari malformation (congenital, with abnormal posterior fossa). Low-lying cerebellar tonsils in intracranial hypotension (reversible with treatment) may be mistaken as congenital Chiari. Intracranial hypotension may also worsen cerebellar tonsillar descent in patients with congenital Chiari.
- Patients with Ehlers-Danlos Syndrome often have multiple comorbidities
- In some cases, intracranial hypotension may lead to a diagnosis of a Heritable Disorder of Connective Tissue not previously recognized; screening for vascular complications such as thoracic aortic aneurysm or intracranial aneurysm should be considered on a case by cases basis.
Clinical presentations that may be unrecognized as possibly secondary to intracranial hypotension
- Subdural hematoma
- Dementia
- Parkinsonism or other movement disorders
- Stupor or coma
- Subarachnoid hemorrhage
- Stroke (ischemic or hemorrhagic)
- Superficial siderosis
- Cerebral venous thrombosis
- Reversible cerebral vasoconstriction
- Posterior reversible encephalopathy syndrome
- Spinal manifestations (radiculopathy, myelopathy, syringomyelia, quadriplegia, bibrachial amyotrophy) – large extradural fluid collections usually evident
- Death
Additional diagnostic challenges
- Not every patient with intracranial hypotension has headache; there are many clinical presentations
- Not every headache related to a spinal CSF leak is positional
- Not every patient with a positional headache has a spinal CSF leak
- Lumbar puncture is not required to make the diagnosis
- Normal or high CSF pressures do occur and do not rule out the diagnosis
- Interpretation of imaging requires experience and training
- Normal cranial MRI does not rule out the diagnosis
- Extradural CSF at C1-2 and the cervicothoracic junction are common false localizing signs
- Sensitivity of spinal imaging is inadequate to localize a significant percentage of leaks, even with the most refined techniques, which limits treatment options
- More than one type of spinal imaging and/or repeat imaging is often necessary
Testing to Confirm a Diagnosis of Spinal CSF Leak
Diagnostic testing includes lumbar puncture (not required), cranial (brain) imaging, spinal imaging, and occasionally a nuclear medicine study called a radioisotope cisternogram. Most radiology departments can perform these procedures, however, in cases where a leak cannot be localized, neuroradiology departments that see larger volumes of spinal CSF leak patients may offer the additional expertise with interpretation as well as with optimization of imaging sensitivity. The understanding of anatomic types of leaks has resulted in refined imaging strategies to characterize a leak in a specific patient to guide treatment.
Types of Imaging Used to Diagnose Spinal CSF Leak
CRANIAL IMAGING
Cranial imaging includes both MRI and CT. An MRI of the brain should be done in ALL cases where a spinal CSF leak is suspected. This should be done without and with gadolinium enhancement. CT imaging of the brain is not infrequently ordered when a patient presents to the emergency room with acute onset of severe headache. Subdural fluid collections or subdural hematomas may be seen. MRI is, however, the preferred imaging of the brain for diagnosis.
SPINAL IMAGING
Spinal imaging is performed to localize leaks. It should be emphasized that spinal imaging may not be necessary since many patients respond well to lumbar epidural blood patching. MRI without intrathecal contrast and CT myelography are used most commonly. Digital subtraction myelography is used increasingly. It should be noted that extradural CSF at C1-2 and the cervicothoracic junction are common false localizing signs. Spinal imaging continues to be refined but remains insufficiently sensitive to image about half of suspected spinal CSF leaks. More than one type of spinal imaging and/or repeat imaging is often necessary.
SPINAL MRI
This is magnetic resonance imaging of the spine that includes sequencing that makes CSF appear obvious without the use of intrathecal contrast. Because this is non-invasive, this is often the first type of spinal imaging used.
INTRATHECAL GADOLINIUM-ENHANCED SPINAL MRI
Spinal MRI may also be done following injection of gadolinium into the intrathecal space via lumbar puncture, although this is an off-label use of gadolinium.
CT MYELOGRAM
A CT myelogram involves injecting radiographic contrast into the intrathecal space via lumbar puncture, followed by a CT of the spine. An opening pressure may be measured and CSF may be collected for analysis. Several variables can be manipulated, depending on the circumstances, such as timing of the imaging after the injection of contrast (dynamic, early, delayed), the intrathecal injection of normal saline to raise the intrathecal pressure, positioning of the patient, or the use of digital subtraction imaging (see below).
DYNAMIC CT MYELOGRAM
In this kind of myelogram (an injection of intrathecal contrast + imaging), the CT is performed as the contrast is being injected. This is most commonly used to localize rapid or high-flow spinal CSF leaks. This is also used with the patient side-lying to detect the CSF-venous fistula type of leak.
DIGITAL SUBTRACTION MYELOGRAM (DSM)
A DSM is a myelogram done under fluoroscopy with the additional ability to digitally subtract a pre-contrast image to enhance the visualization of the contrast. This is a dynamic form of imaging. This can be done under general anesthesia to stop breathing for a short time, thereby preventing movement artifact on the imaging. A CT can be done soon after or with a delay. This is used to image rapid leaks, ventral (front of the spinal cord) leaks or leaks not associated with an obvious extrathecal CSF collection, such as a CSF-venous fistula. Positioning may be side-lying, prone or supine.

An image of two different types of spinal CSF leak as seen via digital subtraction myelogram
MR MYELOGRAM
This kind of myelogram involves MR imaging of spine with the use of specific sequencing/weighting (no intrathecal contrast). Extra-dural contrast may be seen with some spinal CSF leaks. In addition, a variety of abnormal spinal cysts may be noted.

An image illustrating diagnostic findings in a patient with intracranial hypotension
LUMBAR PUNCTURE (LP)
An LP may be done to measure the opening pressure and to collect CSF for analysis, but this is not required to make the diagnosis. An opening pressure is often measured at the time of LP for myelography. Normal opening pressure has a reference range of 65 to 195 mm of water. The opening pressure is often <60, and can be unmeasurable or subatmospheric. Normal pressure is not uncommon, however, and does not rule out CSF leaking. High pressures also occur.
RADIOISOTOPE CISTERNOGRAM
The radioisotope cisternogram is a nuclear medicine study that is occasionally used. This can help to confirm the presence of CSF leaking, but is insensitive in localizing leaks.
Diagnostic Findings
There are five findings typically seen on imaging that can be remembered by the mnemonic “SEEPS” when considering the diagnosis of spinal CSF leak.
However, it is important to note that the absence of these findings does not rule out CSF leaking. The lower prevalence of dural enhancement associated with longer duration of symptoms can contribute to underdiagnosis.
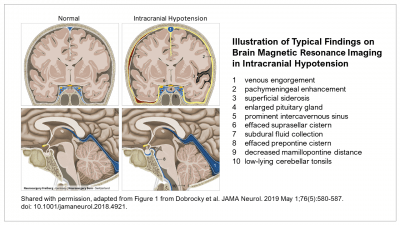
There are additional specific findings that neuroradiologists, neurosurgeons and other clinicians will look for, including decreased mamillopontine distance, effaced prepontine cistern, and superficial siderosis.
The image below features the typical brain MRI findings in patients with intracranial hypotension due to spinal CSF leak.

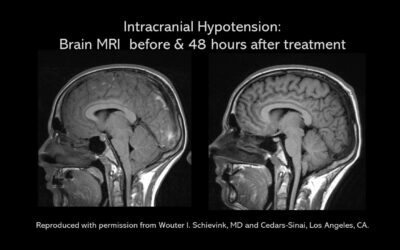
Here is an example of a cranial MRI in a patient with a diagnosis of intracranial hypotension due to spinal CSF leak before and after treatment.
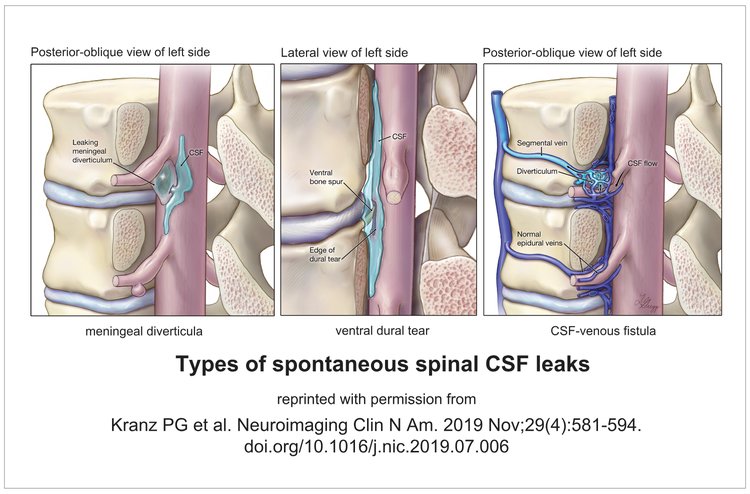
Types of Spontaneous Spinal CSF Leaks
From Classification of Anatomic Types of Spontaneous Spinal CSF Leaks [Neurology. 2016 Aug 16; 87(7) 67379]
Type 1 – dural tear – extradural CSF collection in almost all
1a – ventral CSF leaks [associated with spinal pathology]
1b – posterolateral CSF leaks
Type 2 – meningeal diverticula – extradural CSF collection in ~ 1/4
2a – simple diverticula
2b – complex meningeal diverticula / dural ectasia
Type 3 – CSF-venous fistula – extradural CSF collections absent on CTM
Type 4 – indeterminate – extradural CSF collections in ~ 1/2
This understanding of anatomic leak types has contributed to the evolution of imaging strategies tailored to the suspected leak type. Treatment approach is then planned on the basis of specific leak type and location.
Diagnostic Criteria for Spontaneous Spinal CSF Leaks
The following are some of the established criteria for diagnosis of spinal CSF leak.
Proposed Diagnostic Criteria for Spontaneous Spinal CSF Leaks (2011)
A: Orthostatic headache;
B: The presence of at least one of the following:
low opening pressure (≤60 mm H2O),
sustained improvement of symptoms after epidural blood patching,
demonstration of an active spinal cerebrospinal fluid leak,
cranial magnetic resonance imaging changes of intracranial hypotension (e.g., brain sagging or pachymeningeal enhancement);
C: no recent history of dural puncture; and
D: not attributable to another disorder.
ICHD-3, the International Criteria of Headache Disorders, 3rd edition, 2018
These criteria were based on the proposed criteria published in 2011 (above):
7.2.3 Headache attributed to spontaneous intracranial hypotension
Previously used terms: Headache attributed to spontaneous low CSF pressure or primary intracranial hypotension; low CSF-volume headache; hypoliquorrhoeic headache.
Description: Orthostatic headache caused by low cerebrospinal fluid (CSF) pressure of spontaneous origin. It is usually accompanied by neck stiffness and subjective hearing symptoms. It remits after normalization of CSF pressure.
Diagnostic criteria:
A. Headache fulfilling criteria for 7.2 Headache attributed to low cerebrospinal fluid (CSF) pressure, and criterion C below
B. Absence of a procedure or trauma known to be able to cause CSF leakage1
C. Headache has developed in temporal relation to occurrence of low CSF pressure or CSF leakage, or has led to its discovery2
D. Not better accounted for by another ICHD-3 diagnosis.
Notes:
1. 7.2.3 Headache attributed to spontaneous intracranial hypotension cannot be diagnosed in a patient who has had a dural puncture within the prior month.
2. Dural puncture to measure CSF pressure directly is not necessary in patients with positive MRI signs of leakage such as dural enhancement with contrast.
Comments:
Spontaneous cerebrospinal fluid (CSF) leak has been associated with heritable connective tissue disorders. Patients with CSF leaks should be screened for connective tissue and vascular abnormalities.
While there is a clear postural component in most cases of 7.2.3 Headache attributed to spontaneous intracranial hypotension, it may not be as dramatic or immediate as in 7.2.1 Post-dural puncture headache. Thus, 7.2.3 Headache attributed to spontaneous intracranial hypotension may occur immediately or within seconds of assuming an upright position and resolve quickly (within 1 minute) after lying horizontally, resembling 7.2.1 Post-dural puncture headache, or it may show delayed response to postural change, worsening after minutes or hours of being upright and improving, but not necessarily resolving, after minutes or hours of being horizontal. The orthostatic nature of the headache at its onset should be sought when eliciting a history, as this feature may become much less obvious over time.
In patients with typical orthostatic headache and no apparent cause, and after exclusion of postural orthostatic tachycardia syndrome (POTS), it is reasonable in clinical practice to provide autologous lumbar epidural blood patch (EBP). While EBPs are frequently effective in sealing CSF leaks, the response to a single EBP may not be permanent, and complete relief of symptoms may not be achieved until two or more EBPs have been performed. However, some degree of sustained improvement, beyond a few days, is generally expected. In some cases, sustained improvement cannot be achieved with targeted (to the site of the leak) and/or non-targeted lumbar EBPs, and surgical intervention may be required.
It is not clear that all patients with 7.2.3 Headache attributed to spontaneous intracranial hypotension have an active CSF leak, despite a compelling history or brain imaging signs compatible with CSF leakage. The underlying disorder may be low CSF volume. A history of a trivial increase in intracranial pressure (eg, on vigorous coughing) is sometimes elicited.
Postural headache has been reported after coitus: such headache should be coded as 7.2.3 Headache attributed to spontaneous intracranial hypotension because it is most probably due to CSF leakage.
ICHD-3, Headache attributed to spontaneous intracranial hypotension